According to recent data from Decision Resources, big pharma companies appear to be running out of time as global revenue growth declines and US revenue stagnates. Global year-over-year industry growth was limited to about 3.2 percent in 2010, compared with 3.5 percent in 2009 and 7.5 percent in 2008. Worse yet, US pharma sales year-over-year growth was a mere 0.7 percent in 2010. Decision Resources’ Pharmaview Director Alasdair Milton explains, “The limited growth is not surprising as patent expiries, payer cost-containment strategies and lack of research and development productivity continue to negatively impact the pharmaceutical market.”
Pharma companies are faced with several significant challenges in addition to the stark reality of significant near-term patent expirations for blockbuster drugs. Challenges include competition from generics, increased government regulation, inefficient corporate structures, and lack of R&D productivity. So, what are pharma companies doing to reverse the downward trend?
• Entering into “Pay-for-delay” agreements with generic drug makers
• Emphasizing biologics in new product development over “small molecule” drugs
• Increasing M&A activity to boost pipeline and revenue
• Outsourcing research and development to CROs (Clinical Research Organizations) Diversifying to other sectors such as generics, diagnostics, devices, and niche healthcare
• Focusing on improving R&D productivity
Many of these strategies represent a retreat away from the pharma sector where pipeline success has been declining over the years. The one factor that directly increases the likelihood of bringing new drugs to market is improving R&D productivity. Everyone in the pharma industry agrees the industry is suffering from a productivity problem. And, every pharma company is trying to improve R&D productivity.
Defining and Measuring R&D Productivity
Data compiled by CMR International and IMS Health confirm that more spending on R&D has, ironically, resulted in fewer drug approvals. While drug research spending between 2002 and 2007 doubled, the number of new drug approvals dropped by half. Take Pfizer, the world’s largest research-based pharmaceutical company.. Its annual research budget was about $8 billion, the highest in the industry. Yet only a handful of internally discovered Pfizer drug candidates have come to market during the past decade. Across the industry, consultants, pharma executives and financial analysts point to the disconnect between outsized pharmaceutical R&D budgets and declining productivity in recent years. So, is it realistic to boil down R&D productivity to the number of approved new molecular entities compared to annual R&D budget in any given year?
We believe R&D productivity needs to be defined and measured using a process model that captures all relevant decision variables. In a comprehensive technical paper titled ‘How to Improve Productivity in Pharma’, authors dive deep into R&D productivity defining it as a combination of efficiency and effectiveness. Efficiency is defined as the ratio of inputs (ideas, investments, time and money) to outputs (number of projects in pipeline, products launched) whereas effectiveness is the ability of the R&D system to produce outputs with certain intended and desired qualities (for example, medical value to patients, physicians and payers, and substantial commercial value). We believe this is a much more realistic view of measuring R&D productivity.
Let’s take a look at this R&D productivity model and the key variables that affect productivity.
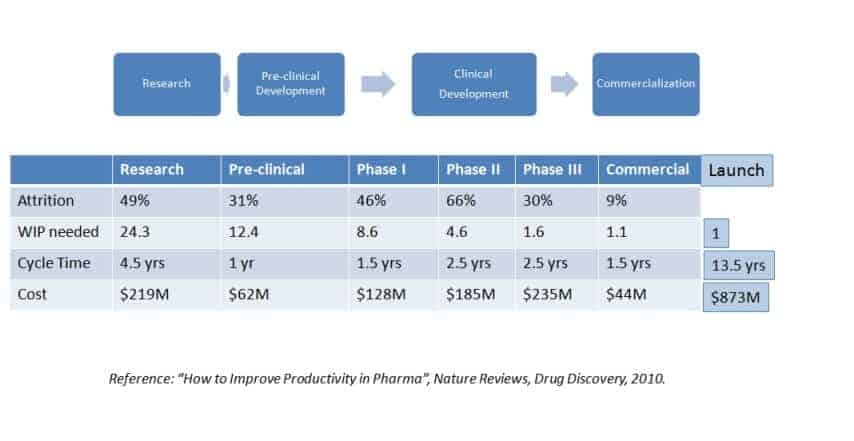
Attrition – the likelihood of a project failing to advance to the next stage in the pipeline. In other words, attrition is one minus the probability of success per stage. It estimated that about 11% of the molecules that enter pre-clinical development stage actually reach the market.
WIP (Work in Process) – the number of molecules in the drug discovery pipeline. According to industry benchmarks on project success rates, there need to be about 53 projects in various stages in the pipeline in order to have one successful launch.
Cycle time – the total time from initial target to selection to commercial launch. According to Pharmaceutical Benchmarking Forum (PBF), it takes anywhere from 11.4 to 13.5 years to bring a new drug to market.
Cost per launch – the sum of project costs per WIP per stage. For example, if there are 12.4 preclinical projects in a pipeline and each costs $5M, the total cost of all preclinical projects in the pipeline portfolios about $62M. It is estimated that, the cost of bringing a new drug to market is $873M.
The outputs presented in this R&D productivity model will vary depending on the R&D processes, inputs, and assumptions of a given pharma or biotech company. However, the model serves as a tool to represent a much more realistic view of the R&D process metrics and analyzing productivity improvement factors.
Based on sensitivity analyses with this R&D model, the authors clearly show that reducing Phase II and Phase III attrition are the two most critical success factors to improving R&D productivity. Yet, the trends are such that Phase II and Phase III attrition rates are increasing due to a variety of reasons including growing drug safety concerns and significant regulatory hurdles to demonstrate benefit-to-risk ratios to patients. As a drug category becomes populated over time with multiple products, each successive new candidate has a higher efficacy (and often safety) hurdle to overcome before being approved. A company with a strategic focus outside of these saturated markets still faces significant attrition in late clinical development. Consequently, the industry has adopted a “fail early, fail fast” strategy in early discovery, setting the safety and efficacy bar high early in preclinical stages of drug testing to avoid costly failure during these expensive clinical efficacy phases of drug development.
Resource Capacity Management: Critical Success Factor for R&D Productivity Improvement
One reasonable solution to dealing with increasing attrition rates in Phase II and Phase III is to increase WIP in Phase I. However, just increasing WIP without managing capacity can significantly increase cycle time and cost. This is especially true when resources are shared and individual subprojects have high variability in their cycle times. In an era where R&D budgets are being slashed and resources are at a premium, greater efficiencies need to be brought to the drug development process than ever before in this industry.
How can WIP be increased without significant increases in cycle time and cost? Of course, there needs to be sufficient WIP in the early stages of the pipeline. From a drug discovery perspective, this means better target selection ,lead optimization, and more predictive ADME and toxicology models. For clinical development, this can be achieved by effective triage, improved pharmacodynamics and the use of surrogate markers and other pharmacodynamics methods to better track efficacy in Phase II and Phase III. Optimizing WIP involves managing risk by selecting and funding portfolio projects with higher likelihoods of success – incorporating WIP optimization with the qualitative improvements to portfolio management listed above is one solution to the efficiency gap that current plagues pharma productivity.
Optimizing WIP (maintaining sufficient levels of projects in various stages of the pipeline) while reducing cycle time and cost is a balancing act. It requires strategic processes and tools for enterprise Resource Capacity Management (ERCM) and Project Portfolio Management (PPM).